I think it’s safe to say that if you’re reading this, you want to be healthy. You want to feel strong and energetic and well. You want to reduce the odds that you will develop a chronic health condition. You like getting good news when you have your blood pressure or cholesterol checked. You might be wondering, does weight loss equal health?
In our society, the dominant, knock-you-over-the-head idea is that to be healthy, we have to lose weight if we are “overweight” or make sure we don’t gain weight if we’re at a “normal” weight. Accordingly, conventional wisdom is that pursuing weight loss will also make us healthier in the long run.
(This is sometimes accompanied by the caveat that, sure, some people try to lose weight in unhealthy ways — laxative abuse, purging, extreme diets — but most of the things people do to lose weight are “healthy.”)
Mmmmmmm…not so much. In reality, there’s less overlap between “pursuit of weight loss” and “pursuit of long-term health” than you think.
Here’s a visual representation that’s more accurate:
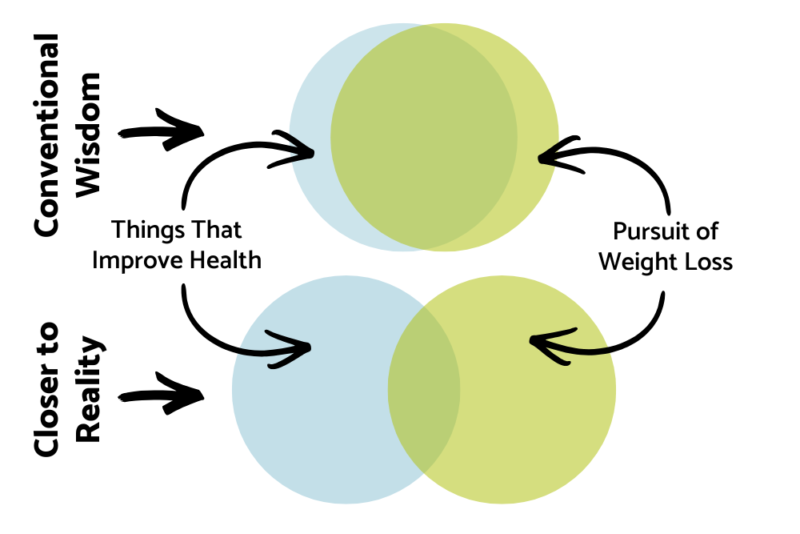
Things that make us healthier (but not necessarily thinner)
There are many, many behaviors that contribute to health, but that don’t necessarily contribute to weight loss:
- Regularly engaging in enjoyable physical activity over the long-term
- Eating a variety of nutritious and enjoyable foods
- Eating when you’re hungry and allowing yourself to eat enough to be satisfied
- Having access to quality, patient-centered healthcare
- Keeping up on preventive healthcare, including screening exams
- Nurturing meaningful social connections
- Prioritizing getting enough quality sleep
- Managing stress levels, through healthy coping mechanisms (this is easier if you also enjoy freedom from oppression and discrimination)
- Cultivating body acceptance
Aspects of dieting that can erode our health and well-being
There are also many, many dieting-related behaviors that can erode health and well-being:
- Taking an all-or-nothing approach to exercise (often based on calorie burn) that increases risk of injury and contributes to “giving up” on exercise for periods of time
- Restricting amounts and/or types of food, which can lead to nutrient shortfalls, rebound binging, food obsession, anxiety, compromised gut health, and possibly an eating disorder
- Avoiding the doctor because you aren’t happy about what you weigh
- Avoiding social gatherings because you “can’t eat that food” or because you don’t want people to see you at your current weight, leading to social isolation.
- Skimping on sleep to make time for extra exercise
- Weight cycling (repeatedly losing and regaining) which over time causes an increase in body fat (known as “fat overshooting”) and a loss of muscle
- Pushing your body below a weight range it wants to be at (weight suppression), leading to a slowed metabolism

The weight-centric approach to health
Our society and our healthcare system operate under a weight-centric approach to health. In other words, the stance that higher weight = poorer health, and weight loss = improved health. Interestingly, the research doesn’t really support this.
The research is clear that
- Having good cardiorespiratory fitness improves health (scientists have identified biological mechanisms that explain this connection)
- Weight stigma and bias, whether directed at us or self-inflicted, is associated with worse health.
We need more research to identify the biological mechanisms explaining the second connection, but one we do know about is that stigma and bias lead to increased stress — including increased levels of the stress hormone cortisol, and ironically can lead to weight gain.
We also know that when stress and increased cortisol are chronic, as it likely is for those in significantly larger bodies (external stigma) and for anyone else who feels that their body is bad and wrong as it is (internal stigma) no matter what size their body is, this plays a causal role in many health conditions. These include cardiovascular disease, type 2 diabetes, and some cancers.
The flaws in weight loss research
Here’s the problem: very little research on weight and health looks at factors like cardiorespiratory fitness or experiences of weight stigma. Let’s say some people in larger bodies do have worse health:
- Could it be because of the physiological and psychological effects of weight stigma and shame?
- Could it be because they don’t exercise, perhaps because they’ve experienced stigma in the gym or rude comments while going for a walk?
If something’s not measured, we can’t assess it, so if researchers don’t ask about exercise habits/fitness levels and external/internal weight stigma, how do they know if it’s really body weight that is responsible for poor health?
Another problem is that weight loss research almost never follows up with participants long enough to discover how many people regained weight, and how much weight. They don’t look at if they’re still exercising, or if their experiences of weight stigma have increased. They don’t know measure the loss of temporary health improvements they experienced while participating in the study.

The weight-inclusive approach to health
A weight inclusive approach makes room for all bodies, without dictating that in order to be healthy, people must change the size of their bodies. This approach focuses on adopting habits known to benefit health — including those I mentioned above — rather than habits that are presumed alter body size or shape.
Even though it’s not a weight-inclusive study, I want to highlight research from the Diabetes Prevention Program (DPP). This study was designed to promote weight loss, using restriction of fat and calories along with increased physical activity to at least 150 minutes per week. Participants in this lifestyle group were more successful at preventing diabetes than a group taking metformin.
Interestingly, the lifestyle group was far more successful at meeting their physical activity goal than their weight loss goal, but the DPP is typically described as evidence that a small amount of weight loss reduces diabetes risk. It could more accurately be described as evidence that regular physical activity reduces diabetes risk.
The weight-inclusive approach fully acknowledges that not all factors that contribute to health are within our personal control, and that the same things that improve health for a thin person improve health for a fat person.
These “things” include the many societal factors that affect our health. These social determinants of health include the conditions in which we live work and play, and those conditions include our access to healthcare and whether we are subjected to bias, stigma and discrimination on the basis of weight, race, gender or other aspects of ourselves.
Making the mental shift
Of course, shifting to a weight-inclusive mindset on a personal level requires a fair degree of “unlearning.” In other words, moving past the idea that weight = health, and also moving past the idea that weight = our value as a human.
Let’s face it, even when we pursue weight loss in the name of “improving health,” there’s that part of us that is seeking society’s approval by achieving — or at least approaching — the thin ideal. In fact, consumer research from the International Food Information Council has found that appearance ranks above health for reasons for starting a diet.
The most meaningful health behaviors are ones that support both physical and psychological well-being. We want to keep doing them regardless of what size we are, and they make our lives bigger and better, not smaller and more stressful.
Having a healthy relationship with food and an effective self-care routine doesn’t require obsession and rigidity and doesn’t lead to anxiety and self-judgment when things don’t go to plan. It’s a journey, not a test. There’s no pass-fail, only learning and curiosity and evolving.
Disclaimer: All information provided here is of a general nature and is furnished only for educational purposes. This information is not to be taken as medical or other health advice pertaining to an individual’s specific health or medical condition. You agree that the use of this information is at your own risk.
Hi, I’m Carrie Dennett, MPH, RDN, a weight-inclusive registered dietitian, nutrition therapist and body image counselor. I offer compassionate, individualized care for adolescents adults of all ages, shapes, sizes and genders who want to heal from an eating disorder, disordered eating or chronic dieting, cultivate an accepting, respectful relationship with their bodies, and gain the freedom to live an authentic, meaningful life without obsessing about food.
Need 1-on-1 help for your nutrition, eating, or body image concerns? Find out how to get started. I’m in-network with Regence BCBS, FirstChoice Health, Providence of Oregon Health Plan and United Healthcare, and can bill Blue Cross and/or Blue Shield insurances in many states. If I don’t take your insurance, I can help you seek reimbursement on your own. To learn more, explore my insurance and services areas page.
 Print This Post
Print This Post





